18.1 – Multiple Linear Regression
Introduction
Last time we introduced simple linear regression:
- one independent X variable
- one dependent Y variable.
The linear relationship between Y and X was estimated by the method of Ordinary Least Squares (OLS). OLS minimizes the sum of squared distances between the observed responses,  and responses predicted
and responses predicted  by the line. Simple linear regression is analogous to our one-way ANOVA — one outcome or response variable and one factor or predictor variable (Chapter 12.2).
by the line. Simple linear regression is analogous to our one-way ANOVA — one outcome or response variable and one factor or predictor variable (Chapter 12.2).
But the world is complicated and so, our one-way ANOVA was extended to the more general case of two or more predictor (factor) variables (Chapter 14). As you might have guessed by now, we can extend simple regression to include more than one predictor variable. In fact, combining ANOVA and regression gives you the general linear model! And, you should not be surprised that statistics has extended this logic to include not only multiple predictor variables, but also multiple response variables. Multiple response variables falls into a category of statistics called multivariate statistics.
Like multi-way ANOVA, multiple regression is the extension of simple linear regression from one independent predictor variable to include two or more predictors. The benefit of this extension is obvious — our models gain realism. All else being equal, the more predictors, the better the model will be at describing and/or predicting the response. Things are not all equal, of course, and we’ll consider two complications of this basic premise, that more predictors are best; in some cases they are not.
However, before discussing the exceptions or even the complications of a multiple linear regression model, we begin by obtaining estimates of the full model, then introduce aspects of how to evaluate the model. We also introduce and whether a reduced model may be the preferred model.
R code
Multiple regression is easy to do in Rcmdr — recall that we used the general linear model function, lm(), to analyze one-way ANOVA and simple linear regression. In R Commander, we access lm() by
Rcmdr: Statistics → Fit model → Linear model
You may, however, access linear regression through R Commander
We use the same general linear model function for cases of multi-way ANOVA and for multiple regression problems. Simply enter more than one ratio-scale predictor variable and boom!
You now have yourself a multiple regression. You would then proceed to generate the ANOVA table for hypothesis testing
Rcmdr: Models → Hypothesis testing → ANOVA tables
From the output of the regression command, estimates of the coefficients along with standard errors for the estimate and results of t-tests for each coefficient against the respective null hypotheses for each coefficient are also provided. In our discussion of simple linear regression we introduced the components: the intercept, the slope, as well as the concept of model fit, as evidenced by R2, the coefficient of determination. These components exist for the multiple regression problem, too, but now we call the slopes partial regression slopes because there are more than one.
Our full multiple regression model becomes

where the coefficients β1, β2, … βn are the partial regression slopes and β0 is the Y-intercept for a model with 1 – n predictor variables. Each coefficient has a null hypothesis, each has a standard error, and therefore, each coefficient can be tested by t-test.
Now, regression, like ANOVA, is an enormous subject and we cannot do it justice in the few days we will devote to it. We can, however, walk you through a fairly typical example. I’ve posted a small data set diabetesCholStatin at the end of this page. Scroll down or click here. View the data set and complete your basic data exploration routine: make scatterplots and box plots. We think (predict) that body size and drug dose cause variation in serum cholesterol levels in adult men. But do both predict cholesterol levels?
Selecting the best model
We have two predictor variables, and we can start to see whether none, one, or both of the predictors contribute to differences in cholesterol levels. In this case, both contribute significantly. The power of multiple regression approaches is that it provides a simultaneous test of a model which may have many explanatory variables deemed appropriate to describe a particular response. More generally, it is sometimes advisable to think more philosophically about how to select a best model.
In model selection, some would invoke Occam’s razor — given a set of explanations, the simplest should be selected — to justify seeking simpler models. There are a number of approaches (forward selection, backward selection, or stepwise selection), and the whole effort of deciding among competing models is complicated with a number of different assumptions, strengths and weaknesses. I refer you to the discussion below, which of course is just a very brief introduction to a very large subject in (bio)statistics!
Let’s get the full regression model
The statistical model is

As written in R format, our model is ChLDL ~ BMI + Dose + Statin.
Note that BMI is ratio scale and Statin is categorical (two levels: Statin1, Statin2). Dose can be viewed as categorical, with five levels (5, 10, 20, 40, 80 mg), interval scale, or ratio scale. If we are make the assumption that the difference between 5, 10, up to 80 is meaningful, and that the effect of dose is at least proportional if not linear with respect to ChLDL, then we would treat Dose as ratio scale, not interval scale. That’s what we did here.
We can now proceed in R Commander to fit the model.
Rmdr: Statistics → Fit models → Linear model
How the model is inputted into linear model menu is shown in Figure 1.
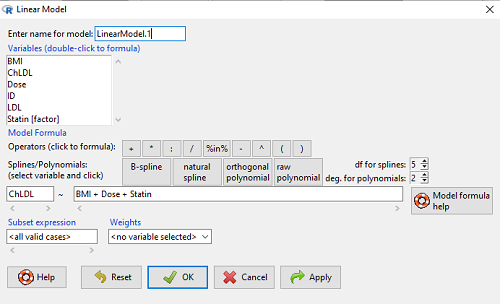
Figure 1. Screenshot of Rcmdr linear model menu with our model elements in place.
The output
summary(LinearModel.1)
Call:
lm(formula = ChLDL ~ BMI + Dose + Statin, data = cholStatins)
Residuals:
Min 1Q Median 3Q Max
-3.7756 -0.5147 -0.0449 0.5038 4.3821
Coefficients:
Estimate Std. Error t value Pr(>|t|)
(Intercept) 1.016715 1.178430 0.863 0.39041
BMI 0.058078 0.047012 1.235 0.21970
Dose -0.014197 0.004829 -2.940 0.00411 **
Statin[Statin2] 0.514526 0.262127 1.963 0.05255 .
---
Signif. codes: 0 '***' 0.001 '**' 0.01 '*' 0.05 '.' 0.1 ' ' 1
Residual standard error: 1.31 on 96 degrees of freedom
Multiple R-squared: 0.1231, Adjusted R-squared: 0.09565
F-statistic: 4.49 on 3 and 96 DF, p-value: 0.005407
Question. What are the estimates of the model coefficients (rounded)?
b0 = intercept = 1.017
b1 = slope for variable BMI = 0.058
b2 = slope for variable Dose = -0.014
b3 = slope for variable Statin = -0.515
Question. Which of the three coefficients were statistically different from their null hypothesis?
Answer: Only the b2 coefficient was judged statistically significant at the Type I error level of 5% (p = 0.0041). Of the four null hypotheses we have for the coefficients (Intercept = 0; b1 = 0; b2 = 0; b3 = 0), we only reject the null hypothesis for Dose coefficient.
Note the important concept about the lack of a direct relationship between the magnitude of the estimate of the coefficient and the likelihood that it will be statistically significant! In absolute value terms b1 > b2, but b1 was not even close to statistical significance (p = 0.220).
We generate a 2D scatterplot and include the regression lines (by group=Statin) to convey the relationship between at least one of the predictors (Fig. 2).
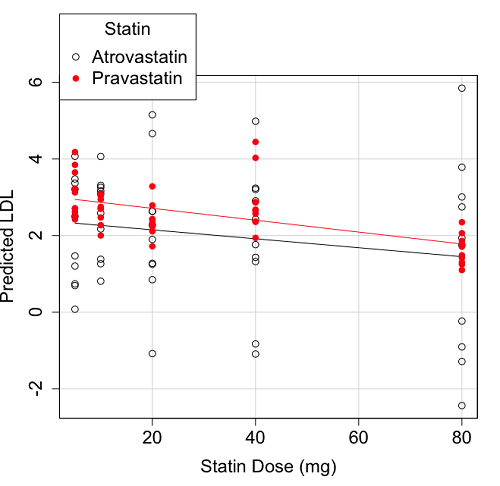
Figure 2. Scatter plot of predicted LDL against dose of a statin drug. Regression lines represent the different statin drugs (Statin1, Statin2).
Question. Based on the graph, can you explain why there will be no statistical differences between levels of the statin drug type, Statin1 (shown open circles) vs. Statin2 (shown closed red circles).
Because we have two predictors (BMI and Statin Dose), you may also elect to use a 3D-scatterplot. Here’s one possible result (Fig. 3).
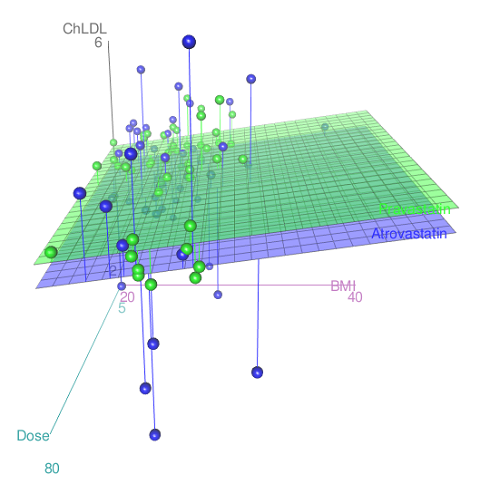
Figure 3. 3D plot of BMI and dose of Statin drugs on change in LDL levels (green Statin2, blue Statin1).
R code for Figure 3.
Graph made in Rcmdr: Graphs → 3D Graph → 3D scatterplot …
scatter3d(ChLDL~BMI+Dose|Statin, data=diabetesCholStatin, fit="linear", residuals=TRUE, parallel=FALSE, bg="white", axis.scales=TRUE, grid=TRUE, ellipsoid=FALSE)
Note: Figure 3 is a challenging graphic to interpret. I wouldn’t use it because it doesn’t convey a strong message. With some effort we can see the two planes representing mean differences between the two statin drugs across all predictors, but it’s a stretch. No doubt the graph can be improved by changing colors, for example, but I think the 2d plot Figure 2 works better). Alternatively, if the platform allows, you can use animation options to help your reader see the graph elements. Interactive graphics are very promising and, again, unsurprisingly, there are several R packages available. For this example, plot3d() of the package rgl can be used. Figure 4 is one possible version; I saved images and made animated gif.
Figure 4. An example of a possible interactive 3D plot; the file embedded in this page is not interactive, just an animation.
Diagnostic plots
While visualization concerns are important, let’s return to the statistics. All evaluations of regression equations should involve an inspection of the residuals. Inspection of the residuals allows you to decide if the regression fits the data; if the fit is adequate, you then proceed to evaluate the statistical significance of the coefficients.
The default diagnostic plots (Fig. 5) R provides are available from
Rcmdr: Models → Graphs → Basic diagnostics plots
Four plots are returned
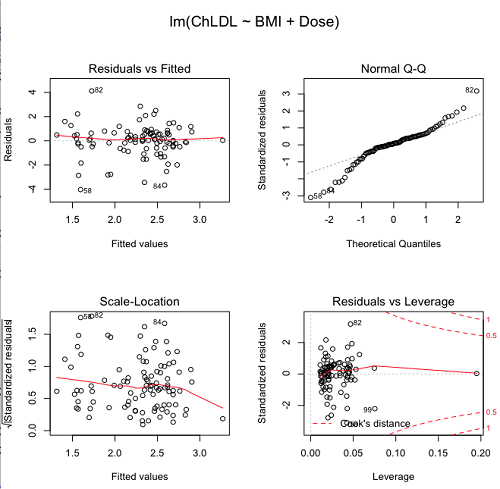
Figure 5. R’s default regression diagnostic plots.
Each of these diagnostic plots in Figure 4 gives you clues about the model fit.
- Plot of residuals vs. fitted helps you identify patterns in the residuals
- Normal Q-Q plot helps you to see if the residuals are approximately normally distributed
- Scale-location plot provides a view of the spread of the residuals
- The residuals vs. leverage plot allows you to identify influential data points.
We introduced these plots in Chapter 17.8 when we discussed fit of simple linear model to data. My conclusion? No obvious trend in residuals, so linear regression is a fit to the data; data not normally distributed Q-Q plot shows S-shape.
Interpreting the diagnostic plots for this problem
The “Normal Q-Q” plot allows us to view our residuals against a normal distribution (the dotted line). Our residuals do no show an ideal distribution: low for the first quartile, about on the line for intermediate values, then high for the 3rd and 4th quartile residuals. If the data were bivariate normal we would see the data fall along a straight line. The “S-shape” suggests log-transformation of the response and or one or more of the predictor variables.
Note that there also seems to be a pattern in residuals vs the predicted (fitted) values. There is a trend of increasing residuals as cholesterol levels increase, which is particularly evident in the “scale-location” plot. Residuals tended to be positive at low and high doses, but negative at intermediate doses. This suggests that the relationship between predictors and cholesterol levels may not be linear, and it demonstrates what statisticians refer to as a monotonic spread of residuals.
The last diagnostic plot looks for individual points that influence, change, or “leverage” the regression — in other words, if a point is removed, does the general pattern change? If so, then the point had “leverage” and thus we need to decide whether or not to include the datum. diagnostic plots Cook’s distance is a measure of the influence of a point in regression. Points with large Cook’s distance values warrant additional checking.
The multicollinearity problem
Statistical model building is a balancing act by the statistician. While simpler models may be easier to interpret and, perhaps, to use, it is a basic truism that the more predictor variables the model includes, the more realistic the statistical model. However, each additional parameter that is added to the statistical model must be independent of all other parameters already in the model. To the extent that this assumption is violated, the problem is termed multicollinearity. If predictor variables are highly correlated, then they are essentially just linear combinations and do not provide independent evidence. For example, one would naturally not include two core body temperature variables in a statistical model on basal metabolic rate, one in degrees Fahrenheit and the other in degrees Celsius, because it is a simple linear conversion between the two units. This would be an example of structural collinearity: the collinearity is because of misspecification of the model variables. In contrast, collinearity among predictor variables may because the data are themselves correlated. For example, if multiple measures of body size are included: weight, height, length of arm, etc., then we would expect these to be correlated, i.e., data multicollinearity.
Collinearity in statistical models may have a number of undesirable effects on a multiple regression model. These include
- estimates of coefficients not stable: with collinearity, values of coefficients depend on other variables in the model; if collinear predictors, then the assumption of independent predictor variables is violated.
- precision of the estimates decreases (standard error of estimates increase).
- statistical power decreases.
- p-values for individual coefficients not trust worthy.
Tolerance and Variance Inflation Factor
Absence of multicollinearity is important assumption of multiple regression. A partial test is to calculate product moment correlations among predictor variables. For example, when we calculate the correlation between BMI and Dose for our model, we get r = 0.101 (P = 0.3186), and therefore would tentatively conclude that there was little correlation between our predictor variables.
A number of diagnostic statistics have been developed to test for multicollinearity. Tolerance for a particular independent variable (Xi) is defined as 1 minus the proportion of variance it shares with the other independent variables in the regression analysis (1 − R2i) (O’Brien 2007). Tolerance reports the proportion of total variance explained by adding the Xi–th predictor variable that is unrelated to the other variables in the model. A small value for tolerance indicates multicollinearity — and that the predictor variable is nearly a perfect combination (linear) of the variables already in the model and therefore should be omitted from the model. Because tolerance is defined in relation to the coefficient of determination you can interpret a tolerance score as the unique variance accounted for by a predictor variable.
A second, related diagnostic of multicollinearity is called the Variance Inflation Factor, VIF. VIF is the inverse of tolerance.

VIF shows how much of the variance of a regression coefficient is increased because of collinearity with the other predictor variables in the model. VIF is easy to interpret: a tolerance of 0.01 has a VIF of 100; a tolerance of 0.1 has a VIF of 10; a tolerance of 0.5 has a VIF of 2, and so on. Thus, small values of tolerance and large values of VIF are taken as evidence of multicollinearity.
Rcmdr: Models → Numerical diagnostics → Variation-inflation factors
vif(RegModel.2) BMI Dose 1.010256 1.010256
A rule of thumb is that if VIF is greater than 5 then there is multicollinearity; with VIF values close to one we would conclude, like our results from the partial correlation estimate above, that there is little evidence for a problem of collinearity between the two predictor variables. They can therefore remain in the model.
Solutions for multicollinearity
If there is substantial multicollinearity then you cannot simply trust the estimates of the coefficients. Assuming that there hasn’t been some kind of coding error on your part, then you may need to find a solution. One solution is to drop one of the predictor variables and redo the regression model. Another option is to run what is called a Principle Components Regression. One takes the predictor variables and runs a Principle Component Analysis to reduce the number of variables, then the regression is run on the PCA components. By definition, the PCA components are independent of each other. Another option is to use ridge regression approach.
Like any diagnostic rule, however, one should not blindly apply a rule of thumb. A VIF of 10 or more may indicate multicollinearity, but it does not necessarily lead to the conclusion that the linear regression model requires that the researcher reduce the number of predictor variables or analyze the problem using a different statistical method to address multicollinearity as the sole criteria of a poor statistical model. Rather, the researcher needs to address all of the other issues about model and parameter estimate stability, including sample size. Unless the collinearity is extreme (like a correlation of 1.0 between predictor variables!), larger sample sizes alone will work in favor of better model stability (by lowering the sample error) (O’Brien 2007).
Questions
- Can you explain why the magnitude of the slope is not the key to statistical significance of a slope? Hint: look at the equation of the t-test for statistical significance of the slope.
- Consider the following scenario. A researcher repeatedly measures his subjects for blood pressure over several weeks, then plots all of the values over time. In all, the data set consists of thousands of readings. He then proceeds to develop a model to explain blood pressure changes over time. What kind of collinearity is present in his data set? Explain your choice.
- We noted that
Dosecould be viewed as categorical variable. ConvertDoseto factor variable (fDose) and redo the linear model. Compare the summary output and discuss the additional coefficients.- Use Rcmdr: Data → Manage variables in active data set → Convert numeric Variables to Factors to create a new factor variable
fDose. It’s ok to use the numbers as factor levels.
- Use Rcmdr: Data → Manage variables in active data set → Convert numeric Variables to Factors to create a new factor variable
- We flagged the change in LDL as likely to be not normally distributed. Create a log10-transformed variable for
ChLDLand perform the multiple regression again.- Write the new statistical model
- Obtain the regression coefficients — are they statistically significant?
- Run basic diagnostic plots and evaluate for
Data set
| ID | Statin | Dose | BMI | LDL | ChLDL |
| 1 | Statin2 | 5 | 19.5 | 3.497 | 2.7147779309 |
| 2 | Statin1 | 20 | 20.2 | 4.268 | 1.2764831106 |
| 3 | Statin2 | 40 | 20.3 | 3.989 | 2.6773769532 |
| 4 | Statin2 | 20 | 20.3 | 3.502 | 2.4306181501 |
| 5 | Statin2 | 80 | 20.4 | 3.766 | 1.7946303961 |
| 6 | Statin2 | 20 | 20.6 | 3.44 | 2.2342950639 |
| 7 | Statin1 | 20 | 20.7 | 3.414 | 2.6353051933 |
| 8 | Statin1 | 10 | 20.8 | 3.222 | 0.8091810801 |
| 9 | Statin1 | 10 | 21.1 | 4.04 | 3.2595985907 |
| 10 | Statin1 | 40 | 21.2 | 4.429 | 1.7639974729 |
| 11 | Statin1 | 5 | 21.2 | 3.528 | 3.3693768458 |
| 12 | Statin1 | 40 | 21.5 | 3.01 | -0.8271542022 |
| 13 | Statin2 | 20 | 21.6 | 3.393 | 2.1117204833 |
| 14 | Statin1 | 10 | 21.7 | 4.512 | 3.1662377996 |
| 15 | Statin1 | 80 | 22 | 5.449 | 3.0083296182 |
| 16 | Statin2 | 10 | 22.2 | 4.03 | 3.0501301624 |
| 17 | Statin2 | 40 | 22.2 | 3.911 | 2.6460344888 |
| 18 | Statin2 | 10 | 22.2 | 3.724 | 2.9456555243 |
| 19 | Statin1 | 5 | 22.2 | 3.238 | 3.2095842825 |
| 20 | Statin2 | 10 | 22.5 | 4.123 | 3.0887629267 |
| 21 | Statin1 | 20 | 22.6 | 3.859 | 5.1525478688 |
| 22 | Statin1 | 10 | 23 | 4.926 | 2.58482964 |
| 23 | Statin2 | 20 | 23 | 3.512 | 2.2919748394 |
| 24 | Statin1 | 5 | 23 | 3.838 | 1.4689995606 |
| 25 | Statin2 | 20 | 23.1 | 3.548 | 2.3407899756 |
| 26 | Statin1 | 5 | 23.1 | 3.424 | 1.2043457967 |
| 27 | Statin1 | 40 | 23.2 | 3.709 | 3.2381790892 |
| 28 | Statin1 | 80 | 23.2 | 4.786 | 2.7486432463 |
| 29 | Statin1 | 20 | 23.3 | 4.103 | 1.2500819426 |
| 30 | Statin1 | 40 | 23.4 | 3.341 | 1.4322916002 |
| 31 | Statin1 | 10 | 23.5 | 3.828 | 1.3817551192 |
| 32 | Statin2 | 10 | 23.8 | 4.02 | 3.0391874265 |
| 33 | Statin1 | 20 | 23.8 | 3.942 | 0.8483284736 |
| 34 | Statin2 | 20 | 23.8 | 2.89 | 1.7211634664 |
| 35 | Statin1 | 80 | 23.9 | 3.326 | 1.9393460444 |
| 36 | Statin1 | 10 | 24.1 | 4.071 | 3.0907410326 |
| 37 | Statin1 | 40 | 24.1 | 4.222 | 1.3223045884 |
| 38 | Statin2 | 10 | 24.1 | 3.44 | 2.472222941 |
| 39 | Statin1 | 5 | 24.2 | 3.507 | 0.0768171794 |
| 40 | Statin2 | 20 | 24.2 | 3.647 | 2.4257575585 |
| 41 | Statin2 | 80 | 24.3 | 3.812 | 1.7105748759 |
| 42 | Statin2 | 40 | 24.3 | 3.305 | 1.9405724055 |
| 43 | Statin2 | 5 | 24.3 | 3.455 | 2.5022137646 |
| 44 | Statin2 | 5 | 24.4 | 4.258 | 3.2280077893 |
| 45 | Statin1 | 5 | 24.4 | 4.16 | 3.4777470262 |
| 46 | Statin2 | 80 | 24.4 | 4.128 | 2.0632471844 |
| 47 | Statin1 | 80 | 24.5 | 4.507 | 3.784421647 |
| 48 | Statin1 | 5 | 24.5 | 3.553 | 0.6957091748 |
| 49 | Statin2 | 10 | 24.5 | 3.616 | 2.6998703189 |
| 50 | Statin2 | 80 | 24.6 | 3.372 | 1.3004010967 |
| 51 | Statin2 | 80 | 24.6 | 3.667 | 1.4181086606 |
| 52 | Statin2 | 5 | 24.7 | 3.854 | 3.1266706892 |
| 53 | Statin1 | 80 | 24.7 | 3.32 | -1.2864388279 |
| 54 | Statin2 | 5 | 24.7 | 3.756 | 2.4236635094 |
| 55 | Statin1 | 40 | 24.8 | 4.398 | 2.907472945 |
| 56 | Statin2 | 40 | 24.9 | 3.621 | 2.3624285593 |
| 57 | Statin1 | 10 | 25 | 3.17 | 1.264656476 |
| 58 | Statin1 | 80 | 25.1 | 3.424 | -2.4369077381 |
| 59 | Statin2 | 10 | 25.1 | 3.196 | 2.0014648648 |
| 60 | Statin2 | 80 | 25.2 | 3.367 | 1.1007041451 |
| 61 | Statin1 | 80 | 25.2 | 3.067 | -0.2315398019 |
| 62 | Statin1 | 20 | 25.3 | 3.678 | 4.6628661348 |
| 63 | Statin2 | 5 | 25.5 | 4.077 | 2.6117051224 |
| 64 | Statin1 | 20 | 25.5 | 3.678 | 2.6330531096 |
| 65 | Statin2 | 5 | 25.6 | 4.994 | 4.1800816149 |
| 66 | Statin1 | 20 | 25.8 | 3.699 | 1.8990314684 |
| 67 | Statin1 | 10 | 25.9 | 3.507 | 4.0637570533 |
| 68 | Statin2 | 20 | 25.9 | 3.445 | 2.3037613081 |
| 69 | Statin1 | 5 | 26 | 4.025 | 2.50142676 |
| 70 | Statin1 | 5 | 26.3 | 3.616 | 0.7408631019 |
| 71 | Statin2 | 40 | 26.4 | 3.937 | 2.5733214297 |
| 72 | Statin2 | 40 | 26.4 | 3.823 | 2.3638394785 |
| 73 | Statin1 | 10 | 26.7 | 4.46 | 2.1741977546 |
| 74 | Statin2 | 5 | 26.7 | 5.03 | 3.845271327 |
| 75 | Statin2 | 10 | 26.7 | 3.73 | 2.7088955103 |
| 76 | Statin2 | 10 | 26.7 | 3.232 | 2.2726268196 |
| 77 | Statin1 | 80 | 26.8 | 3.693 | 1.751169214 |
| 78 | Statin2 | 80 | 27 | 4.108 | 1.8613104992 |
| 79 | Statin2 | 40 | 27.2 | 5.398 | 4.0289773539 |
| 80 | Statin2 | 80 | 27.2 | 4.517 | 2.3489030399 |
| 81 | Statin2 | 20 | 27.3 | 3.901 | 2.7900467077 |
| 82 | Statin1 | 80 | 27.3 | 5.247 | 5.8485450123 |
| 83 | Statin2 | 80 | 27.4 | 3.507 | 1.2478629747 |
| 84 | Statin1 | 20 | 27.4 | 3.807 | -1.0799279924 |
| 85 | Statin2 | 80 | 27.6 | 3.574 | 1.48678931 |
| 86 | Statin1 | 40 | 27.8 | 4.16 | 2.4277532799 |
| 87 | Statin2 | 20 | 28 | 4.501 | 3.2846482963 |
| 88 | Statin2 | 5 | 28.1 | 3.621 | 2.6990067113 |
| 89 | Statin1 | 40 | 28.2 | 3.652 | -1.0912561688 |
| 90 | Statin2 | 40 | 28.2 | 4.191 | 2.8742307203 |
| 91 | Statin2 | 40 | 28.4 | 5.791 | 4.4454535731 |
| 92 | Statin1 | 40 | 28.6 | 4.698 | 3.2028737773 |
| 93 | Statin1 | 5 | 29 | 4.32 | 4.0707532197 |
| 94 | Statin2 | 10 | 29.1 | 3.776 | 2.7512805004 |
| 95 | Statin2 | 5 | 29.2 | 4.703 | 3.6494895215 |
| 96 | Statin2 | 40 | 29.9 | 4.128 | 2.8646910266 |
| 97 | Statin1 | 40 | 30.4 | 4.693 | 4.9837039826 |
| 98 | Statin1 | 20 | 30.4 | 4.123 | 2.2738979752 |
| 99 | Statin1 | 80 | 30.5 | 3.921 | -0.9034376511 |
| 100 | Statin1 | 10 | 36.5 | 4.175 | 3.3114366758 |